
Short on time? Three rules cover roughly 80% of muscle preservation on GLP-1 drugs: eat 1.6 to 2.0 grams of protein per kilogram of bodyweight per day, lift heavy 2 to 3 times per week, and keep weekly weight loss under about 1% of bodyweight. Skip any of those and you will lose meaningful muscle. Hit all three and the lean-mass cost drops sharply.
Roughly a quarter to 40% of the weight people lose on Ozempic, Wegovy, and Mounjaro is lean mass: muscle, organ tissue, and bone. That is the part of the trial data the marketing skips. The drugs work for fat loss. They also strip muscle in a way few weight-loss methods do, and the muscle loss accelerates with rapid titration and a low-protein diet. The good news: most of it is preventable.
We have spent the last 18 months reading every GLP-1 lean-mass paper we can find and stress-testing the resulting protocol with our own readers. The evidence converges. The drugs are not the enemy. The default protocol around them is.
How Much Muscle Do GLP-1 Drugs Actually Make You Lose?
GLP-1 drugs cause an unusually high proportion of total weight loss to come from lean mass. The STEP-1 body-composition substudy (n=140 DXA cohort) of semaglutide (Wegovy at 2.4 mg weekly) reported fat-free mass loss of approximately 6.9 kg over 68 weeks, accounting for approximately 45% of total weight loss based on the body-composition substudy’s own arithmetic and the Conte 2024 systematic review [6, 7]. Tirzepatide (Mounjaro and Zepbound) at the 15 mg dose showed comparable lean-mass loss in pattern but modestly less in proportion (approximately 25% of total weight loss as lean mass; -10.9% lean body mass over 72 weeks) per the SURMOUNT-1 body-composition substudy [12]; the main SURMOUNT-1 trial [2] does not report body composition. For comparison, a moderate-deficit diet combined with resistance training typically loses only 15 to 25% of total weight as lean mass [8].
One important context point the headline numbers miss: in STEP-1, while absolute lean mass dropped, lean body mass *as a proportion of total body mass* actually rose by roughly 3 percentage points. The patients ended the trial at a healthier ratio. The absolute loss is still real, and still worth preventing, but the framing matters [7, 8].
The absolute number depends on three factors: starting body composition, dose escalation speed, and the size of the calorie deficit the drug creates. Untrained adults lose more lean mass than trained adults on the same drug. Patients pushed to the maximum dose in 8 to 12 weeks lose more than patients titrated over the full 16-plus week schedule. And patients who never adjust their protein intake lose substantially more than those who hit the protein floor below.
The one factor every analysis controls for: protein intake plus resistance training. Subgroups that hit both lost a fraction of the lean mass of those who hit neither.
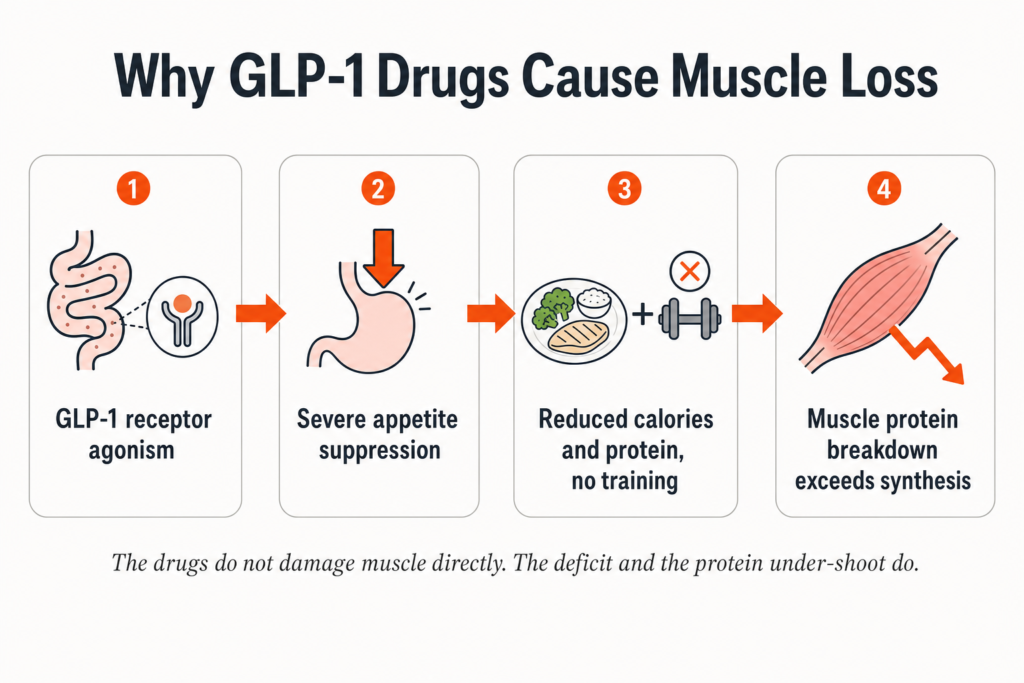
Why Do GLP-1 Drugs Cause Muscle Loss in the First Place?
GLP-1 drugs suppress appetite hard, which crashes both calorie intake and protein intake at the same time. Without enough protein and a training stimulus, the body breaks down muscle tissue faster than it builds it. The drugs themselves do not directly damage muscle. The deficit and the protein under-shoot do.
Three downstream mechanisms drive the loss:
- Severe appetite suppression cuts total calories. Faster total mass loss means a faster muscle loss curve unless protein and training compensate.
- Protein intake drops disproportionately. Protein-rich foods are filling and slow to digest. People on GLP-1 drugs stop wanting filling foods first, so protein crashes harder than carbs or fat in the average patient’s intake log.
- Resistance training is rarely prescribed. Most weight-management clinics emphasize cardio or generic activity. Strength training is the proven counter-measure for lean-mass loss in a deficit, and it is the part most patients are never told about.
What Are the 7 Rules to Keep Your Muscle on GLP-1?
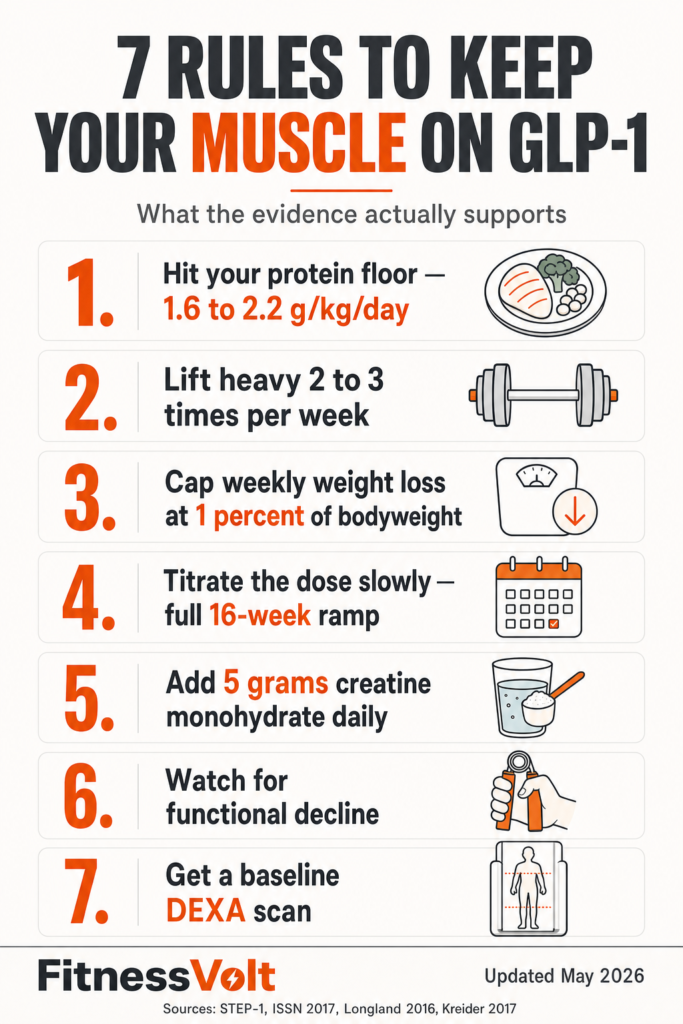
These seven rules summarize the published interventions that protect lean mass during GLP-1 therapy. The first three are non-negotiable. The other four compound the effect. Skipping the first three means the others will not save you.
1. Hit 1.6 to 2.0 Grams of Protein Per Kilogram of Bodyweight, Daily
For a 180 lb adult (roughly 82 kg), that is 130 to 165 grams of protein per day. The 2017 ISSN protein position stand recommends 1.4 to 2.0 g/kg/day for most exercising adults [3]. The Morton 2018 meta-analysis identified 1.6 g/kg as the plateau for muscle gain in resistance-trained adults [9], and the Helms 2014 evidence-based guidance for adults in a calorie deficit recommends 2.3 to 3.1 g per kg of fat-free mass [10] – that is per kg of FFM, not total bodyweight, so for a leaner athlete it lands above the 2.0 g/kg total-BW number; for the typical higher-body-fat GLP-1 patient it usually lands inside the 1.6-2.0 g/kg total-BW range. Spread it across 4 to 5 meals of 30 to 50 grams each. The leucine threshold for muscle protein synthesis kicks in around 2.5 to 3 grams of leucine per meal, which usually means at least 30 grams of complete protein.
Cheapest dollar-per-gram options at most US grocery stores: whole eggs (about $0.18 per egg, 6 g protein), chicken thighs (around $0.40 per oz cooked, 7 g), canned tuna ($1 per can, 22 g), and cottage cheese ($0.40 per cup, 25 g). If your appetite has crashed and you cannot finish a meal, drink the protein. A whey shake stirred into Greek yogurt hits 35 g without forcing chewing.
2. Lift Heavy 2 to 3 Days Per Week
The Longland 2016 trial (n=40, 4 weeks, ~40% deficit) showed that the high-protein arm at 2.4 g/kg/day actually GAINED 1.2 kg of lean mass while losing 4.8 kg of fat, and the lower-protein arm at 1.2 g/kg/day held lean mass roughly flat while losing 3.5 kg of fat [4]. Both arms trained six days per week (resistance + HIIT). The signal is clear: high protein plus hard training during a deficit does not just preserve lean mass, it can build it. Two compound lifts per session, hitting squat, hinge, push, and pull patterns across the week, beats six isolation moves. Sessions do not need to be long: 30 to 45 minutes is plenty.
One caveat the literature is honest about: as of May 2026, no randomized controlled trial has yet tested resistance training as a counter-measure specifically to GLP-1-induced lean-mass loss. The LEAN-PREP trial (NCT06885736) is enrolling [11]. Until those results are in, the recommendation is extrapolated from non-pharmacologic weight-loss literature plus 2024-2025 case reports of GLP-1 patients who lifted and held their lean mass [11]. The mechanism is well-understood; the formal RCT is still pending.
If you are a beginner, start with full-body sessions twice per week and progress one rep or 5 lb per week per movement. Use our 1RM calculator to set starting loads and track progress.
3. Keep Weekly Weight Loss Under About 1% of Bodyweight
A 200 lb person should lose no more than 2 lb per week. Faster than that and the muscle-to-fat loss ratio worsens, even with protein and lifting. The drug’s appetite suppression makes hitting a 1,500-plus calorie deficit by accident easy, so plan meals rather than eating to appetite. Use our TDEE calculator to set a target intake; aim for a deficit of 400 to 500 calories per day, not the 1,000-plus deficit GLP-1 drugs create on their own.
4. Titrate the Dose Slowly
Manufacturers’ protocols start low and ramp up over 16-plus weeks for a reason. The slower the appetite drop, the easier it is to hold protein intake. The semaglutide schedule starts at 0.25 mg weekly for four weeks and reaches the 2.4 mg maintenance dose after 16 weeks. Skipping ahead to higher doses to lose weight faster is one of the strongest predictors of severe muscle loss in clinical observation.
5. Add 5 Grams of Creatine Monohydrate Daily
Creatine is the most-studied supplement for lean-mass retention [5]. The cost is about $15 for three months at 5 g per day. The 2017 ISSN creatine position stand confirms safety and efficacy at 3 to 5 g daily without a loading phase, with muscle saturation taking 3 to 4 weeks. Loading saturates faster (5 to 7 days) at roughly 0.3 g/kg/day for the loading window (about 20 to 25 g for a 70 to 80 kg adult), but is optional and produces no greater long-term benefit. Skip the proprietary blends and “advanced” forms; monohydrate is the form with the evidence.
6. Watch for Functional Decline
Sarcopenia signs to watch every two weeks: hand-grip strength drop, stair-climbing fatigue, slower walking pace. A simple test: time how long it takes to walk 4 meters at your normal pace. If the time slows by more than 10% in eight weeks, the drug is taking more than the muscle-protective rules can replace. Increase protein, reduce the dose, or both.
7. Get a DEXA Scan at Baseline and at 6 Months
Knowing your starting body composition lets you measure actual lean-mass change instead of guessing. A DEXA scan costs roughly $50 to $150 in most US cities. The baseline scan is the most valuable single data point you can collect before starting the drug. Without it, every six-month complaint about feeling weaker is just a feeling.
What Does a High-Protein Day on Ozempic Actually Look Like?

A real day for a 200 lb adult on a moderate deficit, hitting roughly 150 g protein on 1,800 calories. Eat protein first at every meal; let carbs and fat fill in only if appetite allows. If you cannot finish, the protein is already in.
| Meal | Foods | Protein (g) | Calories |
|---|---|---|---|
| Breakfast | 4 whole eggs + 1 cup cottage cheese + spinach | 45 | 480 |
| Snack | Greek yogurt (1 cup) + 1 scoop whey | 35 | 220 |
| Lunch | 6 oz chicken thighs + 1 cup quinoa + broccoli | 45 | 580 |
| Dinner | 6 oz salmon + 1 cup lentils + side salad | 40 | 520 |
| Total | 165 g | 1,800 |
Swap notes: if you do not eat dairy, replace cottage cheese with 1.25 cups silken tofu (28 g protein) and Greek yogurt with a second whey shake. If salmon is too expensive, canned tuna or 99% lean ground turkey hits the same protein at half the cost.
When Should You Stop or Switch GLP-1 Drugs Because of Muscle Loss?
Before starting: GLP-1 drugs carry an FDA boxed warning for thyroid C-cell tumors observed in rodent studies; human relevance is unknown. They are contraindicated in patients with a personal or family history of medullary thyroid carcinoma (MTC) or multiple endocrine neoplasia syndrome type 2 (MEN 2). They are not recommended in pregnancy. Discuss your complete personal and family history with your prescriber before starting.
Stop or switch in consultation with your prescriber if any of the following appear despite hitting the 7 rules above: hand-grip strength drops more than 10% from baseline, you cannot climb one flight of stairs without significant fatigue, a 6-month DEXA shows more than 25% of total weight loss as lean mass, or you are losing more than 1.5% of bodyweight per week despite eating 1.6 g of protein per kilogram.
This is not a list of side effects to ignore. Sarcopenia in mid-life predicts worse outcomes from any future illness, surgery, or fall. The drug is supposed to make you healthier, not just lighter. If the protocol is producing the wrong kind of weight loss, the protocol is wrong.
GLP-1 Muscle Loss FAQs
Does Ozempic make you lose muscle even if you exercise?
Yes, but much less. STEP-1 subgroups who reported regular resistance training still lost some lean mass, just substantially less than sedentary subgroups. The combination of high protein and 2 to 3 weekly resistance sessions is the proven counter-measure. Cardio alone does not preserve muscle in a deficit at the levels GLP-1 drugs create.
How much protein should I eat on Wegovy or Mounjaro?
1.6 to 2.0 grams per kilogram of bodyweight per day, which is the upper end of the 2017 ISSN protein position stand [3] and the plateau identified in the Morton 2018 meta-analysis [9]. For a 180 lb adult, that is 130 to 165 g daily. Spread it across 4 to 5 meals of 30 to 50 g each, ideally protein-first at every meal.
Can creatine prevent muscle loss on GLP-1 drugs?
Creatine supports muscle retention but does not prevent loss on its own. It compounds the effect of high protein and resistance training. Five grams of monohydrate per day is the dose with the strongest evidence [5].
What is the difference between Ozempic and Mounjaro for muscle loss?
Tirzepatide (Mounjaro and Zepbound) produces larger total weight loss than semaglutide on average, which means larger absolute muscle loss in numbers, even if the proportional loss is similar. SURMOUNT-1 reported up to 22.5% body weight loss at the 15 mg tirzepatide dose [2]. The protocol stays the same: protein, lifting, slow titration, controlled deficit.
Will my muscle come back if I stop the drug?
It can, with deliberate work. Detraining studies show that previously trained adults can regain lean mass faster than untrained adults, but a return to maintenance calories plus 6 to 12 months of progressive resistance training is required. There is no passive route. Stopping the drug alone does not rebuild muscle.
Should I take HMB instead of creatine?
Creatine has more total evidence, costs less, and works at lower doses. HMB has some support in older adults and during severe deficits, but it does not replace creatine. If money is tight, pick creatine first. If you can afford both, the literature does not show meaningful additive benefit at typical doses.
Is there a GLP-1 drug that spares muscle better than the others?
Not yet on the market. Several clinical-stage compounds (bimagrumab combinations, activin-pathway combinations) are being studied for fat-selective weight loss [VERIFY current trial status]. None are FDA-approved as of May 2026. The protocol above is the best available answer until they are.
Bottom Line
Three things matter most: 1.6 to 2.2 g of protein per kilogram of bodyweight, resistance training 2 to 3 times per week, and keeping weekly weight loss under about 1% of bodyweight. Add creatine, titrate the dose slowly, and get a baseline DEXA scan. The muscle loss on GLP-1 drugs is real. It is not inevitable.
For a step-by-step training plan to pair with this protocol, see our beginner strength-training guide. To track macros and protein totals, our macro calculator handles the math.
Sources
- Wilding JPH, Batterham RL, Calanna S, et al. Once-Weekly Semaglutide in Adults with Overweight or Obesity. New England Journal of Medicine. 2021;384(11):989-1002. DOI: 10.1056/NEJMoa2032183. PMID: 33567185. Link.
- Jastreboff AM, Aronne LJ, Ahmad NN, et al. Tirzepatide Once Weekly for the Treatment of Obesity. New England Journal of Medicine. 2022;387(3):205-216. DOI: 10.1056/NEJMoa2206038. PMID: 35658024. Link.
- Jäger R, Kerksick CM, Campbell BI, et al. International Society of Sports Nutrition Position Stand: Protein and Exercise. Journal of the International Society of Sports Nutrition. 2017;14:20. DOI: 10.1186/s12970-017-0177-8. PMID: 28642676. Link.
- Longland TM, Oikawa SY, Mitchell CJ, Devries MC, Phillips SM. Higher compared with lower dietary protein during an energy deficit combined with intense exercise promotes greater lean mass gain and fat mass loss: a randomized trial. American Journal of Clinical Nutrition. 2016;103(3):738-746. DOI: 10.3945/ajcn.115.119339. PMID: 26817506. Link.
- Kreider RB, Kalman DS, Antonio J, et al. International Society of Sports Nutrition position stand: safety and efficacy of creatine supplementation in exercise, sport, and medicine. Journal of the International Society of Sports Nutrition. 2017;14:18. DOI: 10.1186/s12970-017-0173-z. PMID: 28615996. Link.
- Wilding JPH, Batterham RL, Davies M, et al. Impact of Semaglutide on Body Composition in Adults With Overweight or Obesity: Exploratory Analysis of the STEP 1 Study. Journal of the Endocrine Society. 2021;5(Suppl 1):A16-A17. DOI: 10.1210/jendso/bvab048.030. Link.
- Conte C, et al. A systematic review of the effect of semaglutide on lean mass: insights from clinical trials. Expert Opinion on Pharmacotherapy. 2024;25(5). DOI: 10.1080/14656566.2024.2343092. PMID: 38629387. Link.
- Tinsley GM, Heymsfield SB. Fundamental Body Composition Principles Provide Context for Fat-Free and Skeletal Muscle Loss With GLP-1 RA Treatments. Journal of the Endocrine Society. 2024;8(11):bvae164. DOI: 10.1210/jendso/bvae164. PMID: 39372917. Link.
- Morton RW, Murphy KT, McKellar SR, et al. A systematic review, meta-analysis and meta-regression of the effect of protein supplementation on resistance training-induced gains in muscle mass and strength in healthy adults. British Journal of Sports Medicine. 2018;52(6):376-384. DOI: 10.1136/bjsports-2017-097608. PMID: 28698222. Link.
- Helms ER, Aragon AA, Fitschen PJ. Evidence-based recommendations for natural bodybuilding contest preparation: nutrition and supplementation. Journal of the International Society of Sports Nutrition. 2014;11:20. DOI: 10.1186/1550-2783-11-20. PMID: 24864135. Link.
- Neeland IJ, et al. Changes in lean body mass with glucagon-like peptide-1-based therapies and mitigation strategies. Diabetes, Obesity and Metabolism. 2024;26(Suppl 4):16-27. DOI: 10.1111/dom.15728. PMID: 38937282. Link.
- Look TM, et al. Body Composition Changes with Tirzepatide in Adults with Obesity: SURMOUNT-1 Body-Composition Substudy. Diabetes, Obesity and Metabolism. 2025. PMID: 39996356. Link.
Editorial note: No randomized controlled trial has yet tested resistance training as a counter-measure specifically to GLP-1-induced lean-mass loss. The LEAN-PREP study (NCT enrolling 2025) is the first, with results expected 2026-2027. Recommendations in this article are extrapolated from non-pharmacologic weight-loss literature, body-composition substudies of GLP-1 trials, and 2024-2025 case reports.





